

1.0 The Confusing World of a PCOS Diagnosis
Living with PCOS can feel like trying to solve a puzzle with missing pieces. The symptoms often seem unrelated, leaving you to wonder what's truly going on. You might be experiencing:
- Irregular or heavy periods
- Persistent acne and oily skin
- Frustrating weight gain, especially around the belly
- Hair growth on the face, chest, or back (hirsutism)
- Thinning hair on your head
- Challenges with fertility
If any of this sounds familiar, please know this: you are not alone. PCOS affects an incredible one in ten women. It's a spectrum condition, and you don't need to have all the symptoms to be impacted by the underlying imbalance.
The first and most important thing to understand is that the name "Polycystic Ovarian Syndrome" is incredibly misleading. It puts the focus squarely on the ovaries, suggesting it's a problem that starts and ends there. But that's not the real story.
2.0 Why We're Taught to Focus on the Ovaries
It's completely understandable why doctors, patients, and families all focus on the ovaries when they hear "PCOS." The name itself points us in that direction. Conventional medicine often treats PCOS as a purely gynecological (GYN) issue, a problem to be managed by specialists who focus on the female reproductive system.
This approach seems logical on the surface, but it misses the bigger picture entirely.
“...conventional medicine usually views PCOS as a GYN problem... because I mean the word ovaries is in it so it must be a GYN issue right? but it actually isn't...”
This common misunderstanding is the primary reason why so many women are given medications to manage individual symptoms without ever being told how to fix the underlying cause. But what if the cysts on the ovaries aren't the cause of the problem, but just another symptom?
3.0 The Big Reveal: PCOS is a "Whole System" Issue
Here is the single most important shift in understanding you can make: PCOS is not a GYN problem. It is a systemic issue that involves your entire body.
Our bodies are not a collection of separate parts operating in isolation. They are deeply interconnected systems. A problem that shows up in one area (like your ovaries) is often an expression of a much deeper, system-wide imbalance. This perspective is the absolute key to truly understanding—and beginning to heal—PCOS.
For the vast majority of women with this diagnosis, the hormonal chaos, the cysts, and the frustrating symptoms are all downstream effects of one primary issue. And that issue isn't found in the reproductive system at all. It's found in how your body manages energy from the food you eat. It’s time to meet the real driver of the problem: a hormone called insulin.
4.0 Meet the Real Driver: An Insulin Story
For most women, the root cause of PCOS has very little to do with the ovaries. It’s an insulin problem. Let's break down what that means with a simple story.
4.1 Insulin's Day Job
Insulin is a crucial hormone whose main job is to manage your blood sugar. When you eat a meal, the food is broken down into glucose (sugar), which is your body's primary fuel. Insulin's job is to take that glucose from your blood and deliver it to your cells for energy.
4.2 The "Uber" Analogy for Insulin Resistance
To make this crystal clear, let's think of it like a ride-sharing service for your body.
- The Players:
- Insulin is the Uber driver.
- Glucose (sugar from your food) is the passenger.
- Your body's cells are the destination (like a house or office).
- The Perfect Trip: You eat a meal. An Uber driver (insulin) efficiently picks up a passenger (glucose) from the bloodstream and successfully drops it off at its destination (a cell). The cell uses the glucose for energy. Everything works perfectly.
- The Problem Starts: Now, imagine you're eating many carb-heavy meals and snacks throughout the day. More and more passengers (glucose) are waiting for a ride. The cells, however, are already full. They lock their front doors and say, "No more visitors, we have enough energy!"
- The Traffic Jam: The Uber drivers (insulin) are now stuck driving around with passengers (glucose) they can't drop off. The body senses the traffic jam of glucose in the blood and thinks the solution is to call more Ubers. It releases even more insulin. This state of having too much insulin is called hyperinsulinemia. This constant flood of sugar and insulin in the blood is toxic and is the first step toward developing pre-diabetes and Type 2 diabetes.
- The Conflict: This standoff—where the high levels of insulin are trying desperately to drop off glucose, but the cells are refusing to accept it—is what we call insulin resistance.
- Where Does It All Go? The body is smart and doesn't want all that toxic sugar floating in the blood, so it starts storing it in other places. This excess energy gets converted and stored as:
- Belly fat
- High cholesterol
- High triglycerides
If you've struggled with weight that feels impossible to lose despite your best efforts, please know there is a biological reason for it—this is not a failure of willpower.
4.3 The Hormone Domino Effect
This is the critical link. In a woman's body, high levels of circulating insulin send a direct signal to the ovaries. That signal tells the ovaries to do one specific thing: produce more testosterone.
All women have and need testosterone, but when insulin resistance pushes its production into overdrive, a hormonal imbalance is created that leads directly to the classic symptoms of PCOS.
5.0 Connecting the Dots: From Insulin to PCOS Symptoms
The excess testosterone triggered by high insulin is the direct cause of many of the most visible and distressing PCOS symptoms.
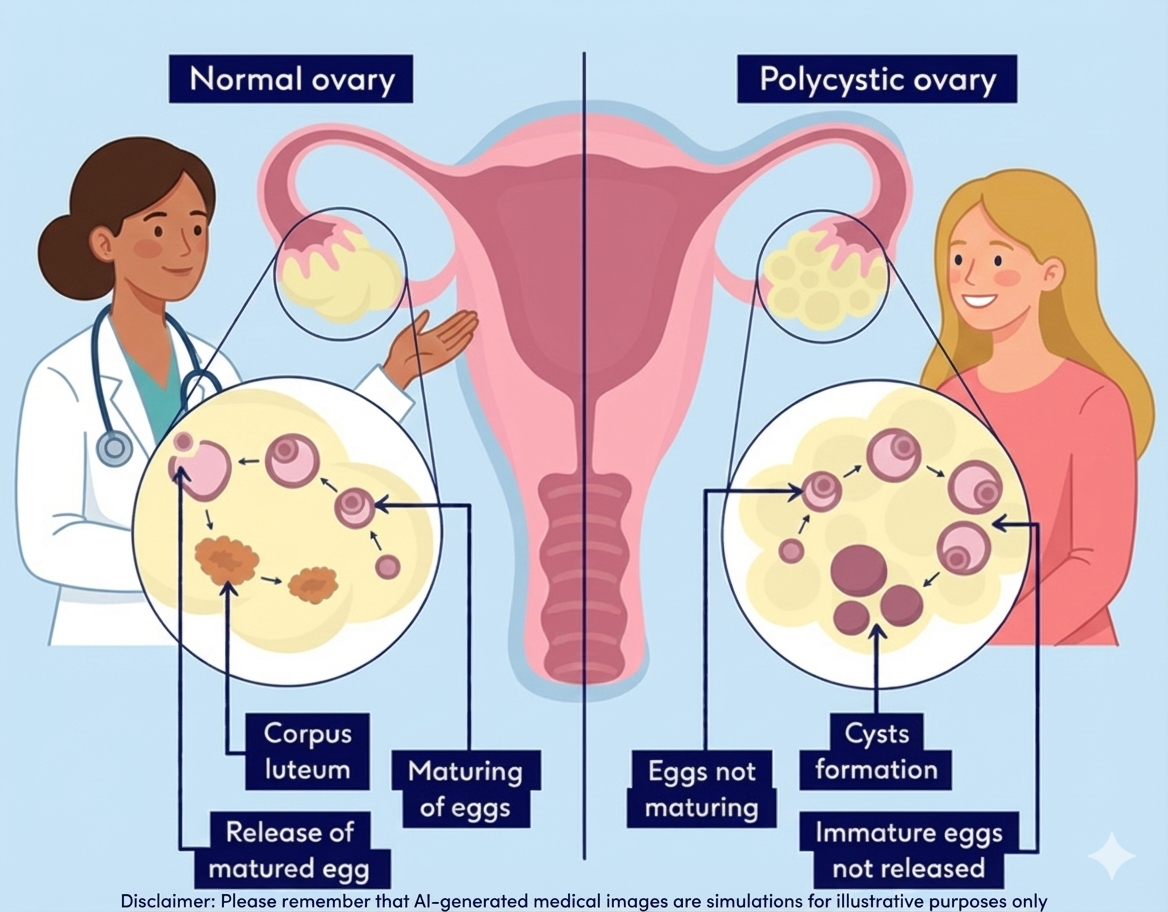
So, where do the "polycystic" ovaries come in? The high testosterone also disrupts the normal development of eggs during your cycle. Instead of maturing fully for ovulation, the eggs can get stuck in a premature state and become small, undeveloped cysts.
This is a crucial point: the cysts are a symptom of the upstream insulin and testosterone problem, not the root cause.Focusing only on the cysts is like mopping up a flooded floor without ever turning off the overflowing faucet.
6.0 Two Paths to Treatment: Masking Symptoms vs. Fixing the Cause
Understanding that PCOS is primarily an insulin problem reveals two very different approaches to managing it.
6.1 The Symptom Management Path
This is the conventional route, which focuses on managing the downstream symptoms. This often involves medications like:
- Birth Control Pills: To force a regular period.
- Spironolactone: To block the effects of high testosterone on skin and unwanted facial hair.
- Metformin: Here is the biggest clue of all, often hidden in plain sight. Metformin is a diabetes medication used to help the body handle insulin better. If you've been prescribed Metformin, you were given a powerful hint that your PCOS is a metabolic issue, even if no one took the time to explain that connection to you.
These medications can provide relief, but they don't address the fundamental "why." They are excellent for mopping the floor, but they never turn off the tap.
6.2 The Root Cause Path
This approach goes straight to the source. The goal isn't to fight your hormones; it's to fix the insulin signaling that threw them off balance in the first place. The primary goal is to teach your body to become insulin sensitive again, so it no longer needs to flood your system with insulin.
Making these changes can feel daunting, especially when you've been taught the opposite for so long. The goal is progress, not perfection.
The main tools for this are powerful lifestyle changes:
- Timed Eating (Intermittent Fasting): This simply means creating a consistent window for eating and fasting. A common method is 16:8, where you eat all your meals within an 8-hour window (e.g., 11 AM to 7 PM) and fast for 16 hours (most of which is overnight while you sleep). This gives your insulin levels a chance to come down and reset.
- Low-Carb Diet: This is about being smart with carbohydrates, not eliminating them. It means reducing your intake of starchy and sugary foods that cause big insulin spikes—think donuts, french fries, pasta, and pizza. It does notmean avoiding healthy, fiber-rich carbs. As one doctor wisely put it, “no one out here is overdosing on Broccoli.”
- Targeted Supplements: Certain supplements can support this process. Inositol, for example, is well-studied for helping cells become more responsive to insulin. However, supplements are partners to nutrition, not replacements for it.
Rethinking Exercise and Fuel
For years, women with PCOS have been told to "eat less, exercise more," but this advice can often backfire.
- The Problem with Over-Exercising: Intense, high-impact workouts (like long-distance running or some HIIT classes) can be a major stressor on the body. This can raise your stress hormone, cortisol, making it harder to lose weight and further disrupting your hormonal balance. Many women find they finally see progress when they switch to lower-impact exercises like walking, Pilates, yoga, or strength training.
- The Danger of Under-Eating: Severely restricting calories or skipping meals sends a threat signal to your body. It thinks a famine is coming and responds by slowing down your metabolism and shutting down non-essential functions—like your reproductive system—to conserve energy. This is the opposite of what you need to heal. Eating enough, especially protein and healthy fats, is crucial.
Navigating Real Life
Sticking to a new lifestyle can be tough, especially in social situations. The key is to have a strategy. Focus on a protein-rich breakfast to stabilize your blood sugar for the day. When you go to a party, offer to bring a healthy dish you know you can eat. And most importantly, remember that one day of indulgence will not undo months of progress. It’s about consistency, not perfection.
7.0 What If It's Not an Insulin Problem?
It's important to know that a smaller percentage of women with PCOS do not have classic insulin resistance. For these women, the hormonal imbalance may be driven by other root causes, such as:
- Chronic Inflammation
- An imbalanced gut microbiome (the world of bacteria living in your digestive system)
- Adrenal Stress / Cortisol Imbalance
Even in these cases, the core principle remains the same. The goal is always to find and address the “why” behind the hormonal cascade. It’s about customized nutrition and lifestyle changes that target your specific trigger, not just taking a pill to mask a symptom.
8.0 Your Path Forward
If there is one thing I hope you take away from this, it is this: PCOS is not a life sentence of unmanageable symptoms.
For the majority of women, it is a metabolic condition rooted in insulin resistance—and that is something you have a tremendous amount of influence over. Your body has an incredible capacity to heal when given the right support.
Start asking "why." “Seek guidance from practitioners who are committed to finding the root cause of your health issues, rather than simply masking symptoms.By understanding the real story of what's happening in your body, you empower yourself to move from being a passenger to being the driver—a true "Game Changer"—on your journey back to health.